
Following a few more than slightly disconcerting conversations about implantable contact lenses recently, Moorfields Ken Pullum has asked us to publish a paper clarifying the points to consider before undertaking this procedure.
The expression, an implantable contact lens (ICL) describes a type of intra ocular lens (IOL) implanted into the eye. IOLs are used extensively to optimise vision following cataract surgery replacing the natural crystalline lens. An implantable contact lens is the term given to an IOL which does not replace the cataractous natural crystalline lens but is placed on the front surface of a healthy, clear crystalline lens in order to modify its optical power.
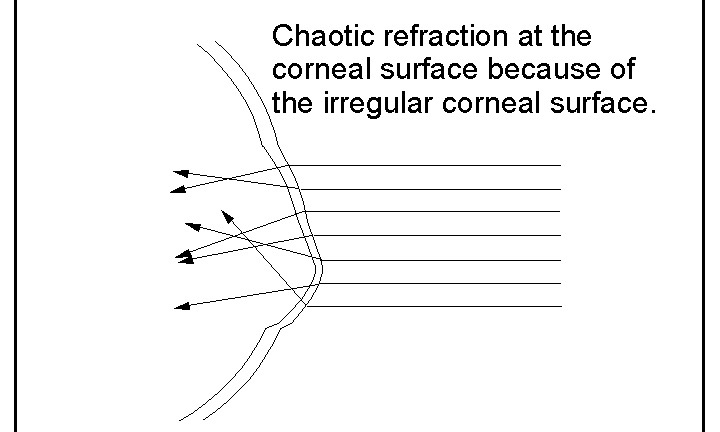
A spectacle prescription is made up of a spherical and a regular astigmatic element which is the difference in curvature of two principal meridians at right angles to each other. Best corrected spectacle vision with keratoconus is blurred and distorted because the corneal surface is not symmetrical about the visual axis. The astigmatism can be very high and is irregular because the principal meridians are not at right angles.
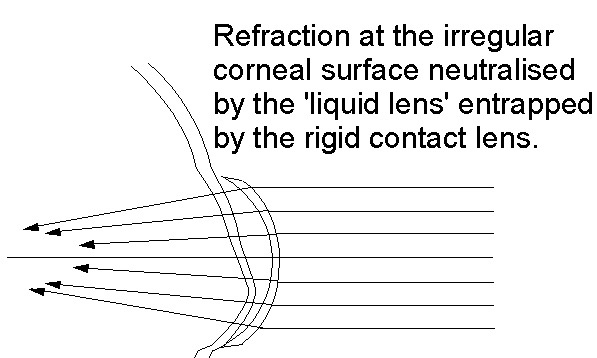
A rigid contact lens retains a fluid reservoir between itself and the front surface of the cornea. The front of the lens becomes the new principal focussing surface with minimal further refraction at the cornea because the refractive index of the fluid reservoir is very close to that of the cornea. There may also be some added regularisation of the corneal surface if there is some contact between the lens and the cornea, provided this can be tolerated. Thus a rigid contact lens corrects most of the keratoconic distortions without the need to incorporate a toroidal element.
Figure 1 illustrate the chaotic refraction at the corneal surface with keratoconus and Figure 2 how it is regularised with the fluid reservoir retained behind a rigid contact lens
The fundamental principle of contact lens management and visual rehabilitation for keratoconus simply is not addressed by an ICL which provides no optical neutralisation of the front surface of the cornea at all. For this reason, an ICL cannot be expected to provide a better level of acuity than the best possible with a spectacle lens.
In fact, it could well be not as good as the best spectacle correction because the light passing through the cornea is irregular when it is incident on the ICL which can only be manufactured to focus symmetrical light.
Furthermore, if a toroidal ICL is used, the intention is to correct the astigmatism which is determined by evaluation of the corneal topography. The fluid reservoir retained by a rigid contact lens neutralises the corneal surface astigmatism whether it is regular or irregular, and the contact lens cannot be constructed not to do this. The astigmatism is effectively corrected twice when a rigid contact lens is used for an eye already fitted with a toroidal ICL. The astigmatic component incorporated into the ICL needs to be corrected again, but this is technically very difficult to achieve with rigid lenses. The higher the astigmatic component of the ICL, the more difficult it is to achieve a result with a contact lens.
Can an ICL ever be indicated for keratoconus?
Yes, under some circumstances. But only if the keratoconus is low grade, there is functional vision with spectacles, there is a clearly established cessation of progression, the spectacle correction gives reasonable vision, and it is established that contact lenses are so poorly tolerated that they cannot be worn usefully at all.
If the spectacle correction does provide functional vision but is so strong that it causes a high level of aberration or distortion, an ICL may offer an improved image quality. However, spectacle refraction with keratoconus is often not well defined or reproducible, and even in a case of stable keratoconus, is subject to change at a future date. The optical specification of the ICL can only be determined by the corneal topography and the spectacle refraction, so can only be prescribed according to the result at the time of the assessment.
Are combined complex surgical procedures possible with ICLs?
Yes, and it seems to be an option that is offered.
Corneal cross linking
While some people describe an improvement following corneal cross linking (CXL) reducing the surface irregularity is not usually stated as an objective. However, CXL may be offered in conjunction with an ICL to reduce progression and future refractive changes.
Surgery to modify or improve corneal topography
There must be some additional means of neutralising the irregular corneal surface for an ICL to be effective in more advanced keratoconus. Corneal refractive procedures or insertion of intracorneal ring segments (ICRSs) may be offered in conjunction with an ICL and CXL also carried out for improved long term stability.
Refractive surgery
Laser refractive surgery is widely available for the treatment of regular refractive errors. The process has traditionally been considered contraindicated for keratoconus because substance is removed from an already thinner than normal cornea, so there is a risk that the keratoconus may be further exacerbated. Indeed, an occasional complication for some people with day-to-day myopia who have opted for refractive surgery develop a thinning and distention of the cornea not dissimilar to keratoconus. It is not clear if keratoconus was missed in the pre-operative assessment or if it is an unpredictable rare complication. Either way, it is not surprising there is a reticence to offer refractive surgery as a treatment option for keratoconus. However, if just low grade, and stabilised with CXL, it is being offered for keratoconus and sometimes in association with an ICL.
Intra corneal ring segments
Intracorneal ring segments (ICRSs), usually a pair for each cornea, can be inserted into the corneal stroma modify the corneal topography. INTACS, KeraRings, FerraraRings and MyoRings are four types that have been developed. They have been available for several years but have always divided opinion. The objective is to flatten the peripheral cornea with the intention of regularising the refraction at the corneal surface. It seems unlikely that the visual outcome could be better than the best achievable with contact lenses, but if contact lenses are poorly tolerated, an improvement over unaided vision and best spectacle vision is possible. If some reduction of the corneal topography is achieved with ICRSs, there may be an improved visual outcome with an ICL. To reduce the chance of keratoconus progression, CXL would also have a crucial role.
Figure 3 shows an eye having had ICRSs inserted and an ICL implanted.

Figure 3, published in the Indian Journal of Ophthalmology is an optical coherence tomography (OCT) image illustrating an ICL just vaulting the anterior surface of the crystalline lens. ICRSs have also been inserted into the corneal stroma.
If there are to be three procedures, and if contact lenses are not delivering a satisfactory result, perhaps a deep anterior lamella keratoplasty may be a better option.
Corneal transplantation
A corneal transplant removes the irregular cornea, so an ICL inserted at the time of the transplant would be completely inappropriate. An ICL is a better prospect following a transplant than for pre operated keratoconus as the topography is usually more regular, so a spectacle refraction is more stable once the transplant has finally settled. However, a decision to carry out a further procedure after a transplant would be a major undertaking and not taken lightly.
How should the conversation proceed if ICLs are discussed?
Most people I have met in the keratoconus group are more than capable of understanding the issues involved and can participate in a conversation about the outcome prospects of treatment options.
If an ICL is projected as an alternative to rigid contact lenses, the question to ask is how does the ICL deal with the irregular corneal surface. If the reply is that it works just like any other contact lens, but without the hassle, the best advice is to walk away. An ICL does not work similarly in any way.
If additional surgical procedures are suggested to address the irregular corneal surface, the question is how this is achieved, and what are the realistic risks and benefits.
And finally, if the procedure does not yield a favourable result, what are the prospects for reversal.
To summarise
- Implantable contact lenses should not be mistaken for contact lenses used to rehabilitate keratoconus.
- They do not neutralise or regularise the irregular corneal surface, which is the cornerstone principle of contact lens optical correction.
- The optical correction can only be expected to be something approaching the best achieved with spectacle correction and could be less effective.
- Subsequent rigid contact lens correction may be more complicated, and it is possible that the vision outcome may be worse than contact lens correction alone.
Ken Pullum
June 2021
Email kenpullum@btconnect.com