A Moorfields and UCL Institute of Ophthalmology team led by Daniel Gore have developed a ‘prediction calculator’ to give keratoconus patients a personalised risk calculation to make informed decisions about treatment.
Keratoconus is a condition that causes the cornea to thin and impair vision. It is one of the most common reasons for corneal transplants in younger patients, and usually presents itself in their early teens. While milder cases can be managed by contact lenses or glasses, in more advanced cases a corneal transplant may be required to restore vision. A treatment called corneal cross-linking (CXL) is able to effectively stop disease progression, but is not always suitable.
The calculator creates a unique graph for each eye of each patient based on their individual risk factors to assess their likely prognosis, helping both clinicians and patients to decide when and if to proceed with CXL. This calculator is part of a wider project to offer more personalised management plans to patients to improve outcomes.
Eye experts across the UK are calling for your input into a new survey designed to refresh the James Lind Alliance Sight Loss and Vision research priorities that were first published in 2013.Despite on-going eye research taking place across the world, there are still many questions about the prevention, diagnosis and treatment of sight loss and eye conditions that remain unanswered. Funding for research is limited, so it is important for research funders to understand the unanswered questions of greatest importance to patients, relatives, carers and eye health professionals so that future research can be targeted accordingly.Following a review of the existing eye research priorities by the NIHR Ophthalmology Specialty group and the UK Clinical Eye Research Strategy earlier this year, a survey has been developed to help fine tune which of the 98 potential research questions should be taken forward as part of the refresh.Professor Rupert Bourne, NIHR National Specialty Lead for Ophthalmology said:“It’s almost 10 years since the UK last published its eye research priorities and progress has been made in learning more about each of those 12 key areas that were set at the time. This survey is designed to help us assess whether these are still the right priorities for us to be focusing our attention on, and to delve deeper into some of those, or whether there are new areas of eye research that we now need to make a priority.“We are encouraging all those with an interest in eye health and research to take part in the survey to help shape the direction of future eye research.” The Eye Research Priority survey is open to all eye healthcare professionals and researchers as well as patients, carers and members of the public to participate in; and will be open until 9 August 2022. The survey feedback will inform the final Top 10 updated priorities across different eye sub-specialties.
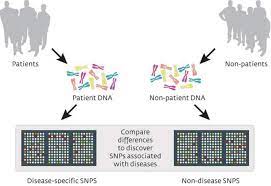
Members will remember the talk given by Professor Alison Hardcastle at our AGM in 2019, updating us on her work as part of the Genome-Wide Association Studies (GWAS). The talk was summarised in our Summer 2019 newsletter.
The authors from UCL Institute of Ophthalmology, Moorfields Eye Hospitaland many other institutions from around the world, have recently published a very significant paper outlining the results of their research to date.
Hi I’m Dale, I have Down syndrome, I’m autistic, I can be extremely challenging because the world doesn’t suit me very well… and I have KC. I will be 40 this year. My abilities are at about a two-year level. I love planes trains rugby and You’ve Been Framed. When I was 5 my birth Mum had the folds by my eyes resected as she didn’t want me to look Downs. What hospital would do that? Later I was adopted into my always and forever family.
When I was 8 I had a squint corrected and instead of the promised left eye and despite a big marker pen arrow on my face, the guy did both eyes “for good measure”. Ruined my good eye. The medical services have always been careless with me! They told Mum to drive me home straight away. I was cold and grey but they said they needed the bed. In the car I stopped breathing I was so congested. When I was 11 a doctor in Spain thought I had leukemia and offered to open me up to see, he said it didn’t matter if I didn’t survive as I was defective anyway….we came home fast. I was fine. When I was 14 I was diagnosed with keratoconus, “severe and progressive.” Our local Hospital had no experience and bandaged my hydrops eye which went septic and stinky. Luckily Mum didn’t stick to their advice and we didn’t go back. She took me to another hospital for assessment in 2000. We had hope and excitement! The Consultant Ophthalmic Surgeon said, ” Visual Acuity is 6/60 with correction (spectacles). This is probably adequate for his needs. Contact Lens fitting is not a sensible option in someone with an intellectual deficit.” Adequate !! Er Nope. Luckily Mum likes a challenge. And the word “lenses ” had been mentioned and being told ‘No’, made her cross! Mum found the kc group and via them, the magical Ken Pullum. Ken saw me for hours and hours and prescribed scleral contacts – I have help managing them and have vision as good as anyone since then 🙂 14/20 distance and symbols smaller than 2mm up close. I was well supervised by Cheltenham General Hospital until staff changes meant they no longer had the expertise. In two weeks, I’m making a return visit to Ken after 25 years. I wonder if Ken will remember us. We remember him; he is my KC superhero.
“I have had suspicions that you might have Keratoconus in your left eye”
In the early 1990s I went to see my optometrist back home in Finland for my annual check
up. I had noticed that sometimes the correction with just glasses left my eyesight especially
on the left side lacking in clarity and focus. Another odd thing was that when I was reading I
was always holding a book within an inch from my eyes. This was the only way I could see
the letters clearly enough to read.
I always remember my reaction to this diagnosis:”Keratoconus? What on earth is that?”.
At that point it felt like everything was about to change for me and little did I know how much!
I had been a patient with this particular optometrist since I was seven years old and she had
always helped me with glasses etc. This though sounded like something entirely different
and well, yes scary.
She told me about it and how the shape of my left cornea was growing conical and this was
why my eyesight was deteriorating. She was not able to say why I had it and I most certainly
had never heard about it before let alone know anyone who had it. My right eye was
unaffected and has remained thankfully like that until now 30 odd years later. Later on I
learned that I do have it in that eye as well, but luckily it never developed further.
I was sent to a local specialist eye store who were experts in contact lenses that same day.
This was also all new to me and to be honest probably kind of scarier in a weird way than
the actual diagnosis had been. I had a sort of quick overview of lenses and was told that my
Keratoconus in my left eye was mild and RGPs were pretty much the only option at that
point. So I was fitted with hard lenses in my eyes.
I have to say that my eyesight improved instantly and it was great to be able to see clearly
once again. It took quite some time to get used to wearing them and taking care of the
lenses – back in those days water was used to clean them! Something that would be a
complete taboo now due to danger of infections. It does make me smile thinking back to
those days. CXL was not even a thing back in those days.
Fast forward a few years and sadly progressing fast in my left eye. After further
appointments, cornea transplant was the only option available and I was referred to the
Helsinki University Hospital for the operation which eventually took place in 1996. This was
quite scary and in those days the internet was still new and getting information about this
was really tricky. There were some discussion forums and websites in existence and I
remember trying to find as much information I possibly could prior to the operation.
My life changed entirely thanks to get gift of sight to a donor in Denmark – yes, I am 1%
Danish now! Healing took quite some time, but my eyesight got better gradually and in the
end I only needed correction with glasses. At that point I had moved to the UK and had to fly
occasionally to some final appointments back home in Finland.
My graft has been a true success story – 27 years and still going strong!! I dont even need
steroids or other eye drops anymore. Sadly though things have not been completely plain
sailing and roughly two years ago my eyesight started getting blurrier with glasses in my left
eye. I went to my optician and was told that they were no longer able to help me as I had
developed scarring in my graft. This was a shock to the system and while waiting for the
referral and eventually appointment at the cornea clinic at my local hospital I was quite
miserable as I was not not able to see well. Working with screens became very tricky, but
thankfully I did get occupational glasses which helped a lot with this problem. Sadly my
appointment got rescheduled a few times and the wait was fairly long. This is why I had
occupational glasses prescribed.
Eventually the appointment arrived and of course it felt anxious waiting to hear if and how
they could help me to see better again. I was given two options at this point – either
keratoplasty to remove scarring with laser or to start using special contact lenses.Due to risk
with keratoplasty I was referred to the contact lens clinic at the hospital. It took three months
to be seen, I am now wearing a mini scleral in my left eye and RGP in my right one. My
vision is great and I can wear the lenses comfortably about 14 hours daily. Fitting process
has been long and currently I am on my fifth pair and very near final fit.
I am so grateful for the NHS and being able to see crystal clear again. Keratoconus certainly can be a tough one to deal with especially as it is not that well known and more awareness is needed for sure. It can be really scary and cause anxiety, but with right information and most importantly professional care it can be much more manageable with a good eyesight. Everyone is different of course, but I am happy to say that I have had the gift of eyesight now twice in my life. There is always hope!
We would like to thank our friends at the National Keratoconus Foundation in America and Keratoconus Australia for organising this competition. Congratulations to our own Ashley Winter for his winning entry.
At our previous Zoom coffee morning, we were treated to an excellent talk by Howard Mailes, a PhD candidate at UCL. He was talking about his research into using artificial intelligence to assist with the initial diagnosis of Keratoconus, and detecting progression.
For the past few years our group has been working with health professionals in Wales where until now, apart from very exceptional cases, it has not been possible to have Cross Linking (CXL) performed by the National Health Service. However, at last we have some good news to report. Crosslinking cross-linking CXL
Health Technology Wales has just issued revised guidance for the use of CXL. Their original report on the topic in 2018 stated that there was insufficient evidence(!) for CXL to be used by the NHS in Wales. The revised guidance now states –
“The evidence supports the routine adoption of corneal cross-linking (CXL) for children and adults with progressive keratoconus. Compared to standard care, CXL slows disease progression and may improve visual acuity. It may also reduce or delay the need for corneal transplantation. Economic modelling suggests that CXL is cost effective on the basis of an assumed sustained clinical benefit for at least 14 years.”
This now needs to translate into CXL being offered in Welsh hospitals (at the moment, only Singleton Hospital in Swansea does) and that is a decision for the Welsh government. Let’s hope that follows swiftly! You can read the full guidance (which includes a submission from the Keratoconus Group) …Here
Update from Anne Klepacz-
I have now had some feedback from my contact at HTW –
“Thank you so much for your contributions to this appraisal – our appraisal panel were particularly moved by the testimony provided from the patient group and have asked me to pass on their thanks. I think this is such a great example of how important this work of engagement with patients and groups such as yourselves is for health technology assessments.”
So I in turn would like to thank all our members and forum users who have talked and posted about their KC experience and more recently their CXL experience. Without your voices, we couldn’t have contributed to the review (it’s just a shame that we weren’t consulted back in 2018!) You’ll find our submission right at the end of the report, in Appendix 4.
A clinical trial in 60 keratoconus patients aged 10-16 years old, most of which were based at the NIHR Clinical Research Facility at Moorfields Eye Hospital, found that a treatment for keratoconus, known as corneal cross linking, was effective at stopping its progression in young patients.
We shall be hosting a presentation of the results of this trial on 9th October 2021, details to follow.
Keratoconus is an eye condition where the normally round, dome-shaped, clear front window of the eye (cornea) progressively thins, causing a bulge to develop. This eventually impairs the ability of the eye to focus properly, potentially causing progressively worsening vision.
It is known that corneal cross-linking treatment can halt keratoconus progression and stabilise vision in adults, but until now we didn’t know the effectiveness of this treatment in young patients. This is particularly important as keratoconus is known to progress faster when the onset is in childhood and early teen years. The results of this study show that treating these younger keratoconus patients with corneal crosslinking is effective in arresting the progression of their disease. The clinical trial results represent evidence previously unavailable which strengthens the cases for making cross-linking available throughout the UK, which at present it is not.
A patient, Anne Klepacz who was the lay representative on the study, through her role as trustee of the Keratoconus Group charity said: “It is very exciting to have the results of this study, giving hard evidence of the effectiveness of corneal crosslinking in young people, and providing reassurance and clarity for both parents and young people with keratoconus. We hope the findings will result in crosslinking becoming widely available throughout the UK.”
Frank Larkin, consultant ophthalmologist at Moorfields Eye Hospital, said: “Our findings suggest that corneal crosslinking should be considered as the first line treatment in progressive keratoconus in young patients. It will be interesting to see the longer term impact of this treatment for these patients and if it means the patients won’t need to wear contact lenses or have a corneal transplantation in later life.”